
Guest article by
Mich Powers, DVM, CCRT
Diplomate of the American College of Veterinary Surgeons -SA
Diplomate of the American College of Sports Medicine & Rehabilitation (canine)
Introduction
Canine Hip Dysplasia (CHD) is the most common orthopedic condition of the dog that results in hip joint inflammation with secondary osteoarthritis (OA). CHD is of complex inheritance, meaning that multiple genes and nongenetic influences (body weight, environment, nutrition) affect the expression of the disease. (Smith GK K. G.-L., 2012).
Normal force, congruency, and load are needed between the femoral head and acetabulum for the coxofemoral joint to develop correctly. Laxity of the coxofemoral joint plays a major role in the development of osteoarthritis (OA) of the hip joint. At birth, the canine hip is normal, if hip laxity is present it leads to subluxation during growth, which then leads to abnormal development of the acetabulum and femoral head. The repetitive subluxation and reduction lead to cartilage erosion and damage to the dorsal acetabular rim, leading to OA. As OA progresses over time decreased range of motion, stiffness, decreased muscling and diminished quality of life can occur. CHD affects millions of dogs each year and is a major concern for pet owners, breeders, working/performance dog owners, and veterinarians.
Being able to obtain an accurate diagnosis and determine risks will help planning whether the surgical procedure may be needed and/or a multimodal medical management approach. A multimodal medical management approach has become more prevalent making significant strides in making pets feel more comfortable and being active.
Etiology and Pathogenesis CHD
Understanding Joint Laxity and what we use to measure it
Joint laxity has been shown to be the primary risk factor for the development CHD the progression of coxofemoral osteoarthritis (Runge JJ, 2010) (Smith GK M. P., 2001) There are two types of joint laxity, passive (non-weight-bearing) and functional (weight-bearing). Passive hip laxity is an estimation of functional hip laxity and what is commonly measured. Functional laxity is the instability that occurs during weight-bearing, resulting in subluxation of the femoral head and abnormal forces across the joint (King, 2017) that precipitates wear and tear on the articular cartilage leading to osteoarthritis. (WH, 1973) Dogs with higher laxity values are at increased risk for developing osteoarthritis compared to dogs with lower laxity values. (Runge JJ, 2010) (Smith GK G. T., 1993) Laxity can be measured radiographically by two methods: the PennHIP distraction index or subjectively on hip extended pelvic radiograph. On physical exam findings, laxity can be assessed subluxation tests.
Radiographic Measurement of Passive Hip Laxity
-
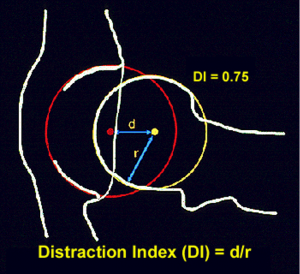
- PennHIP (Distraction Index (DI)) is the measurement of maximal femoral head displacement from the acetabulum when the legs are placed in a neutral position and a distractive force is applied (Fig.1). The DI is calculated by dividing the distance between the geometric center of the femoral head and the geometric center of the acetabulum by the radius of the femoral head. (Fig 2) The Distraction Index (DI) shows that the risk of developing hip OA increases as the distraction index exceeds 0.30. (Runge JJ, 2010) (Kapatikin AS, 2004)

-
- Radiographic subluxation (commonly known as the OFA view/hip extended view) is a subjective assessment of hip laxity obtained from ventral dorsal hip extended radiograph. How well is the femoral head covered (do the hips appear subluxated), is there OA present? (Fig. 3) A study by Heyman et al. (Heyman SJ, 1993), showed that passive hip joint laxity is at its maximum when the joint is placed in a neutral weight-bearing position, which is 15 degrees of extension, 10 degrees of abduction, and 0 degrees of internal/external rotation relative to the plane and axis of the pelvis. When the hip is placed with the hindlimbs into extension as seen on the ventral dorsal hip extended radiograph it produces a “windup” of the coxofemoral joint capsule which limits the lateral movement of the femoral heads thus limiting observable hip laxity.

Physical exam joint subluxation tests
Ortolani, Bardens, and Barlow tests are joint subluxation tests used during a physical exam. The Ortolani test is the most commonly taught and used test. An Ortolani sign is a physical test for hip laxity that correlates roughly with DI. (Puerto DA, 1999) The age at which Ortolani sign becomes predictive of persistent hip laxity and degenerative joint disease is unknown.

When performing the Ortolani test, it is recommended that the dog be sedated or anesthetized because the procedure can be uncomfortable for the patient or if the dog is very tense and good muscling you may get a negative test. The positive Ortolani test involves abducting a subluxated hip until palpable and/or audible click or clunk of the hip is noted. The test can be performed in lateral or dorsal recumbency in the dog. If no palpable or audible reduction of the hip is noted, this is a negative Ortolani test result. (Fig. 4)
Ortolani testing has been shown to provide a 92% to 100% sensitivity for identifying laxity in juvenile dogs > 4 months of age that later developed radiographic signs of hip dysplasia. (Gatineau M, 2014) The Ortolani test may become less pronounced or not present as OA progresses or if the dog is not sedated and very tense you can get a negative test. As osteoarthritis increases in severity, reduction of the subluxated hip becomes less distinct or no longer palpable. A positive Ortolani sign must be interpreted with caution since several studies have reported that a positive Ortolani sign does not necessarily mean that the animal will develop coxofemoral OA. A negative Ortolani sign does not rule out hip dysplasia likely due to false-negative tests. A key thought to remember is that a positive Ortolani should be followed with further diagnostic examination and a negative Ortolani should not be used to rule out hip dysplasia if other signs point towards this disease.
PennHIP Radiographic Screening Program
PennHIP was introduced in 1993 as an evidence-based hip screening method by Dr. Gail Smith of the University of Pennsylvania. PennHIP requires that the dog be heavily sedated or anesthetized and position in dorsal recumbency. Three radiographs are taken of the dog: ventrodorsal hip-extended, compression, and the distraction radiograph. (Fig. 5). (Smith GK B. D., 1990) The certified veterinarian places the custom-designed distraction device is placed between the legs and acts as a fulcrum at the level of the proximal femur, serving to lateralize the femoral heads by applying a small adduction force. (pushing the femoral heads out of the acetabulum).



The distraction index is then calculated by dividing the distance between the centers of the femoral head and acetabulum by the radius of the femoral head. (Fig. 5) A low distraction index (i.e., <0.3) means very tight hips and a high index (i.e., >0.7) means loose hips. Compression (frog-leg) radiographs are also performed to assess achievable congruence. PennHIP requires specific training and mandatory submission of every radiograph performed. The distraction index must be measured by the PennHIP group to allow for consistent readings.
The distraction index (DI) can be calculated as the degree of femoral head subluxation from the acetabulum. A DI score of 0 equates to no subluxation, whereas a DI score of 1 equates to a fully luxated joint.
- Another way to understand distraction index: the number is between 0-1, and if you have a DI of 0.3 think of it as 30% of the femoral head is luxating.
- The higher the DI more subluxation leading to osteoarthritis. DI as a risk factor for the development of OA is comparable to the association of one’s cholesterol level for the risk of developing heart disease. The higher a person’s cholesterol level, the greater risk that the person will develop heart disease. Not all individuals with high cholesterol levels will necessarily develop heart disease in their lifetime. But most people will choose to do things to help keep it low (the non-genetic factors). A key point to remember is tighter hips equate to greater OA resistance. (AIS: Antech Imaging Services, 2016)
The compression radiograph (Fig. 5b) is used to evaluate joint congruency. The hip-extended radiograph (Fig. 5c) is used to evaluate the hip joints for standard evidence of osteoarthritis. The PennHIP method has been shown through multiple studies to be predictive for OA development in animals as young as 16 weeks of age. (Smith GK H. C., 1998)
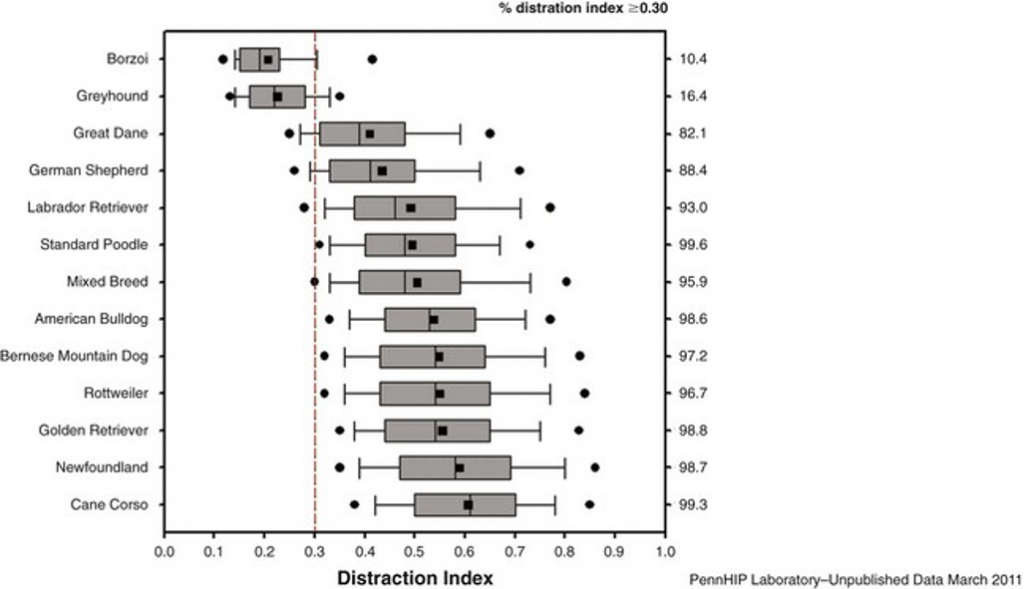
Radiographs taken for PennHIP evaluation must be submitted by the certified veterinarian. This is beneficial to learn what is going on in a particular breed so that there is no selection bias. Furthermore, the PennHip method allows researchers the ability to develop breed-specific DI profiles to provide a better estimate of future breed-related osteoarthritis development. Although there are breed differences, a DI of greater than 0.3 is generally accepted as the cutoff value for osteoarthritis susceptibility. (Fig. 6)
With PennHIP, you have the ability to perform this test as early as 16 weeks of age which then allows for potential surgical intervention (remember there are no surgical procedures to correct hip dysplasia or prevent osteoarthritis from progressing), determining if this puppy should be a working/performance dog or types of activities that may not be ideal for the pet. While many treatments are available for juvenile hip dysplasia, the most performed surgical procedures include juvenile pubic symphysiodesis (JPS), triple pelvic osteotomy (TPO), femoral head and neck ostectomy (FHO), and total hip replacement (THR). My goal in this article is not to say one of these surgeries must be done but to provide information on surgeries potentially available.
- Juvenile Pubic Symphysiodesis, to be effective, must be done in dogs between 12 and 18 weeks of age who have mild or moderate hip laxity (DI ≤0.6). Studies have shown that JPS is effective at increasing coverage of the hip joint however, it has also been shown that it does not eliminate clinical symptoms and progression of osteoarthritis.
- Triple pelvic osteotomy (TPO) and the double pelvic osteotomy (DPO). Both the TPO and DPO are designed to improve acetabular ventro-version and femoral head coverage. Unfortunately, TPO has been associated with a wide variety of complications including progression of hip osteoarthritis, residual or continued lameness, implant failure or urinary complications due to impingement of the urethra. In an effort to decrease complications associated with TPO a different plating technique has been investigated by elimination of the ischial osteotomy (Double pelvic osteotomy) has been proposed. Another disadvantage of the TPO or DPO procedure is the need for exercise restriction and that it only treats one hip joint at a time.
- Femoral head and neck ostectomy (FHO) – salvage procedures that can be done at any age and any size of dog. Performed when medical management has failed.
- Total hip replacement (THR) – THR systems can be categorized into cemented systems, cementless systems (using bone-ingrowth instead of cement), and hybrid systems (combining cemented fixation with cementless for the different components). Aseptic loosening and implant failure due to fatigue failure remain a concern.
Early detection is also extremely valuable in working and performance dog selection. Thousands of dollars are put into the training of these animals, therefore knowing the risk of developing CHD and OA can save money and time training a dog that likely would have to retire early or unable to do its job due to pain. The most common cause of retirement in military working dogs is due to hip OA.
Cavitation on the PennHIP radiograph
Cavitation is a phenomenon that rarely occurs (<4% and usually on one side) during the distraction procedure. As the distractor device imposes a lateral distractive force on the hips, this creation of negative pressure can cause a void to form in the synovial fluid in the joint. This void appears as an air bubble on the radiograph. Cavitation is not painful and does not cause short- or long-term damage to the joint. (LaFond E, 1997). It is the same phenomenon of “cracking” your knuckles.
The appearance of cavitation on a radiograph may be unilateral (one hip), or bilateral (both hips). The cavitation void appears as a dark bubble on the radiograph. Cavitation occurs unilaterally 4.2% of the time and bilaterally 0.27% of the time. The frequency of occurrence is about the same for either hip, occurring 2.2% of the time in the right hip and 2.3% of the time in the left hip. (LaFond E, 1997)
Cavitation is problematic only because it causes the DI measurement to be unreliable. A cavitated joint can have a false increase in the DI, thus cavitation is noted on the PennHIP report. If cavitation is unilateral PennHIP will not assign a DI for the cavitated hip and an interpretation will be derived from the non-cavitated hip. (AIS: Antech Imaging Services, 2016)
If cavitation is bilateral no DI will be generated for either hip and it is recommended that the evaluation be repeated in 24 hours or anytime thereafter.
PennHIP advantages
- Most sensitive test to determine passive hip laxity
- Can be performed on animals as young as ≥16 weeks of age
- Higher heritability rate
- Must submit radiographs for evaluation therefore no selection bias
PennHIP Disadvantages
- Three radiographs under heavy sedation are required
- Training course for certification
- Cost is higher than OFA due to required sedation and 3 radiographic views are taken
Additional radiographic early indicators of osteoarthritis
Caudal curvilinear osteophyte (CCO, or Morgan line) and circumferential femoral head osteophyte (CFHO)
These are two key early radiographic features on the VD hip extended pelvic radiograph that have been reported to represent early osteophyte formation that predict later development of more characteristic signs of osteoarthritis. (Mayhew PD M. P., 2002) (Powers MY B. D., 2004) (Szabo SD, 2007)
- The caudal curvilinear osteophyte (CCO, or Morgan line): is a well-defined linear density on the femoral neck between the greater trochanter and the capital physis in dogs 18 months or older.
- The puppy line is a more subtle opacification of the femoral neck seen in the area of the CCO in young dogs ≤18 months of age. The line is an indistinct radiodense line on the femoral neck similar to the CCO, but is more subtle, more diffuse and shorter than the CCO. It is important to differentiate between the puppy line and the CCO because the puppy line represents an incidental finding that is often gone by 18 months of age and has no correlation with later development of osteoarthritis. (Risler A, 2009) (Mayhew PD M. P., 2002)
In a Lifelong Study in 48 Labrador Retriever dogs, the dogs that had a CCO were 3.7 times as likely to develop radiographic signs of OA than those without a CCO. The dogs were divided into two groups (control-overweight vs. restricted fed): 100% of the overweight dogs with a CCO developed radiographic signs of osteoarthritis and 55% of restricted-fed dogs with a CCO developed radiographic signs of OA. The CCO was the first radiographic change seen in 76% of dogs with osteoarthritis. (Powers MY B. D., 2004)
- Circumferential femoral head osteophyte (CFHO): This is a distinct rim, appearing as a radiopaque line encircling the junction of the femoral head and neck at the site of capsular attachment. (Szabo SD, 2007)
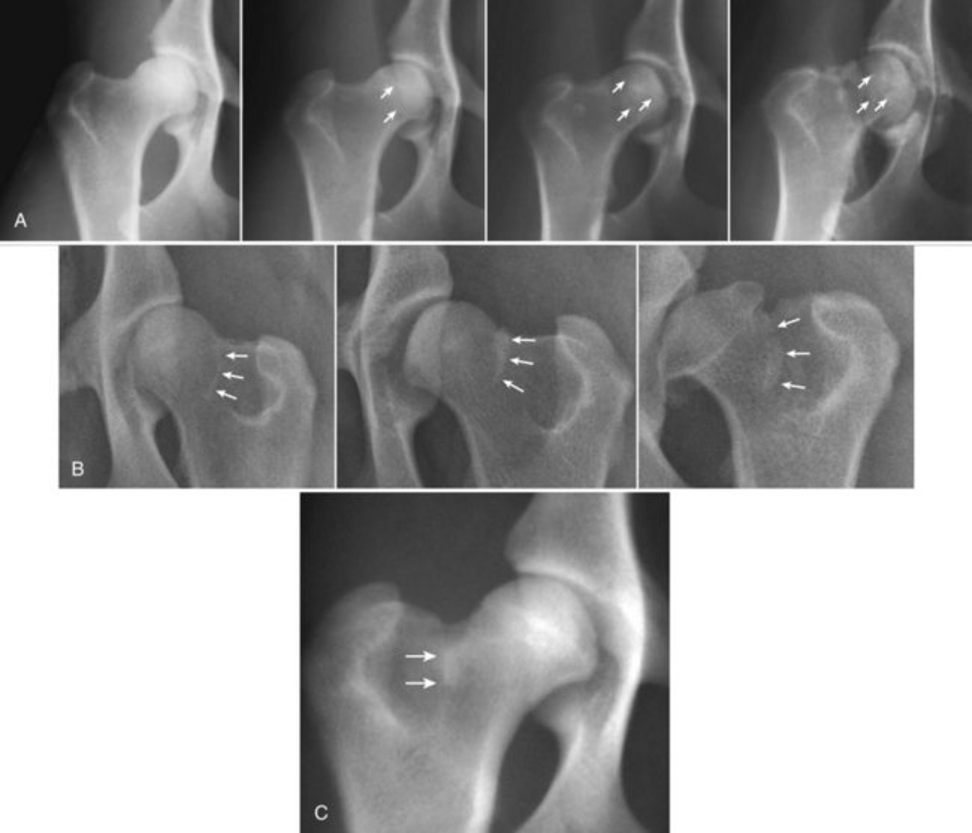
Fig. 7B: CCO well defined linear density on the femoral neck between the greater trochanter and the capital physis. Figure shows the left hip of three different adult dogs, with progressing grades -grade 1, grade 2, and grade 3.
Fig. 7C: The puppy line is more subtle, more diffuse, and shorter than the CCO.
These early radiographic indicator markers, CCO, and CFHO are not yet adopted by any of the hip screening organizations.
Hormonal effects on hip dysplasia and PennHIP
Contrary to popular belief, estrus (being in heat) is of no consequence to hip scoring. A study by Hassinger et al (Hassinger KA, 1997) showed definitively that estrus does not adversely affect the distraction index or any other hip scoring method, including the subjectively-read, hip-extended method. The hormone relaxin remains present up to 8 weeks post whelping (although it varies by breed). Currently, there is no study describing whether relaxin influences DI or any other hip scoring method. It is recommended by PennHIP to be on the safe side and wait 8 weeks post-lactation or 16 weeks post-whelping before hip testing. (AIS: Antech Imaging Services, 2016)
Does the PennHIP procedure damage the hips or cause more pain than the hip extended view? There is no evidence to suggest that the PennHIP procedure is any more harmful than the standard hip-extended procedure. Certainly, in dogs having extreme laxity and pain associated with inflammation and advanced osteoarthritis of hip dysplasia, any manipulation of the hip whether in your general physical exam or standard radiographic views of the hips can potentially cause transient discomfort (1- 2 days). (AIS: Antech Imaging Services, 2016)
Bodyweight
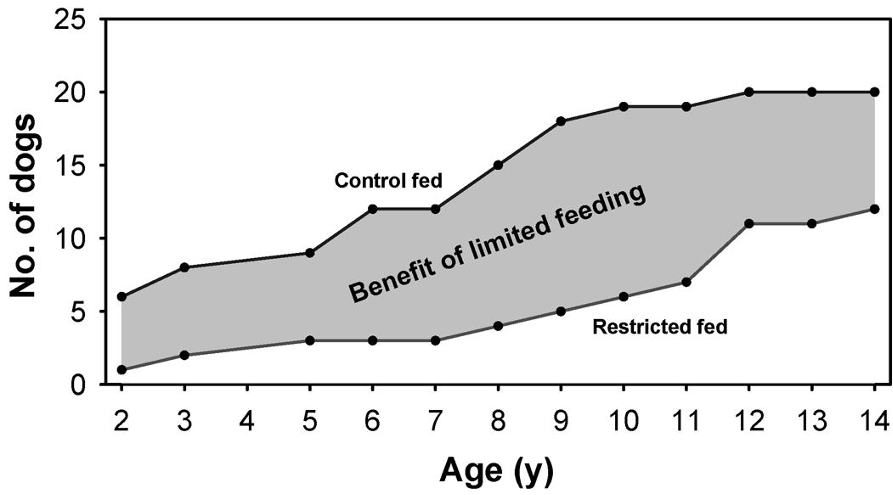
One of the biggest non-genetic factors that can affect hip OA expression and clinical signs. When a dog has OA the damaged cartilage does not resist biomechanical stress as effectively as healthy cartilage. As a result, excessive body weight causes additional mechanical stress on joints, accelerating the degenerative process. Restricting caloric intake minimizes the prevalence, severity, and onset of OA in the coxofemoral joint. (Kealy RD L. D., 1996) (Kealy RD L. D., 2000) (Smith GK & McKelvie PF, 2006) A study by Smith et al showed a cohort of 48 Labrador retrievers divided into two groups followed over their lifetime. The group that was maintained on a diet restriction had delayed onset and reduced severity of hip joint osteoarthritis, thus favorably affecting both length and quality of life. This study also showed that hip osteoarthritis can develop at any time throughout a dog’s life. Fig 8. (Smith GK & McKelvie PF, 2006)
The goal is to maintain these animals at lean body weight, meaning a body condition score for dogs is 4.5 (1–9 scale) or 2.5 -2.7(1–5 scale). There is also evidence that body fat has a metabolic activity that promotes inflammatory reactions within the body, which may contribute to the pathophysiology of OA. Therefore, weight reduction should also have a direct anti-inflammatory effect through the reduction in proinflammatory adipokines. (Harper, 2016). Lean body weight is a vital factor in reducing clinical signs and slowing the progression of OA in dogs.
REFERENCES
(2009, Mar-Apr). Vet Radiol Ultrasound, pp. 1578-66.
Adams WM, D. R. (1998, Jul -Aug). Early detection of canine hip dysplasia: comparison of two palpation and five radiographic methods. J Am Anim Hosp Assoc, pp. 339-47.
AIS: Antech Imaging Services. (2016). Retrieved from Antech Imaging Services: https://antechimagingservices.com/antechweb/fast-facts-behind-the-pennhip-research
Dycus DL, L. D.-L. (2017, July 1). Physical Rehabilitation for the Management of Canine Hip Dysplasia. Veterinary Clinics: Small Animal Practice, pp. 823-850.
Gatineau M, D. J. (2014, Jan 1). Palpation and dorsal acetabular rim radiographic projection for early detection of canine hip dysplasia: a prospective study. Vet Surg, pp. 42-53.
Gordon WJ, C. M. (2003, Sept). The Relationship Between Limb Function and RadiographicOsteoarthrosis in Dogs with Stifle Osteoarthrosis. Vet Surg, pp. 451-4.
Haney PS, L. L. (2020, Aug 1). Effectiveness of PennHIP and Orthopedic Foundation for Animals measurements of hip joint quality for breeding selection to reduce hip dysplasia in a population of purpose-bred detection dogs. J Am Vet Med Assoc, pp. 299-304.
Harper, B. (2016). Current Topics in Canine and Feline Obesity. In M. K. Farcas AK, Veterinary Practice: Small Animal Practice (pp. 785-795). Elseiver.
Hassinger KA, S. G. (1997, Oct). Effect of the oestrus cycle on coxofemoral joint laxity. Vet Comp Orthop Traumatol, pp. 69-74.
Henricson B, N. I. (1966). On the Etiology and Pathogenesis of hip dysplasia: a comparative review. Journal of Small Animal Practice, 673-688.
Heyman SJ, S. G. (1993, Feb). Biomechanical study of the effect of coxofemoral positioning on passive hip joint laxity in dogs. Am J Vet Res, pp. 210-5.
K, L. (VOLUME 47, ISSUE 4, JULY 1, 2017). Juvenile Pubic Symphiodesis. In Veterinary Clinics: Small Animal (pp. 851-863).
Kapatikin AS, G. T. (2004, Feb 15). Comparison of two radiographic techniques for evaluation of hip joint laxity in 10 breeds of dogs. J Am Vet Med Assoc, pp. 542-6.
Kealy RD, L. D. (1996, Dec 31). Five-year longitudinal study on limited food consumption and development of osteoarthritis in coxofemoral joints of dogs. J Amer Vet Med Assoc, pp. 222-225.
Kealy RD, L. D. (2000, Dec 1). Evaluation of the effect of limited food consumption on radiographic evidence of osteoarthritis in dogs. J Amer Vet Med Assoc, pp. 1678-1680.
King, M. (2017). Etiopathogenesis of Canine Hip Dysplasia, Prevalence, and Genetics. In B. J. Harper TA, Veterinary Clinics of North America: Small Animal Practice (pp. 753-767). St. Louis: Elsevier.
LaFond E, S. G. (1997, May 1). Synovial fluid cavitation during distraction radiography of the coxofemoral joint in dogs. J Am Vet Med Assoc, pp. 1294-1297.
Manley PA, A. W. (2007, Jan 15). Long-term outcome of juvenile pubic symphysiodesis and triple pelvic osteotomy in dog with Hip Dysplasia. Journal of American Veterinary Medical Association, pp. 206-210.
Mayhew PD, M. P. (2002, Feb 15). Evaluation of a radiographic caudolateral curvilinear osteophyte on the femoral neck and its relationship to degenerative joint disease and distraction index in dogs. J Am Vet Med Assoc, pp. 472-476.
Mayhew PD, M. P. (2002, Feb 15). Evaluation of a radiographic caudolateral curvilinear osteophyte on the femoral neck and its relationship to degenerative joint disease and distraction index in dogs. J Am Vet Med Assoc., pp. 472-476.
Orthopedic Foundation for Animals. (2020). Retrieved from Orthopedica Foundation For Animals: https://www.ofa.org/diseases/breed-statistics#detail
Paster ER, L. L. (2005). Estimates of prevalence of hip dysplasia in Golden Retrievers and Rottweilers and the influence of bias on published prevalence figures. J Am Vet Med Assoc., 387-392.
Piermattei DL, F. G. (2006). Textbook of Small Animal Orthopedics and Fracture Repar. St. Louis: Elsevier.
Powers MY, B. D. (2004, Jul 15). Use of the caudolateral curvilinear osteophyte as an early marker for future development of osteoarthritis associated with hip dysplasia in dogs. J Am Vet Med Assoc. , pp. 233-237.
Powers MY, B. D. (2004, Jul 15). Use of the caudolateral curvilinear osteophyte as an early marker for future development of osteoarthritis associated with hip dysplasia in dogs. J Am Vet Med Assoc, pp. 233-237.
Powers MY, K. G. (2010, Sept 1). Evaluation of the relationship between Orthopedic Foundation for Animals’ hip joint scores and PennHIP distraction index values in dogs. J Am Vet Med Assoc, pp. 532-41.
Powers MY, M. S. (2005, Oct 1). Prevalence of cranial cruciate ligament rupture in a population of dogs with lameness previously attributed to hip dysplasia: 369 cases (1994-2003). J Am Vet Med Assoc, pp. 1109-1.
Puerto DA, S. G. (1999, Jan 31). Relationships between results of the Ortolani method of hip joint palpation and distraction index, Norberg angle, and hip score in dogs. Journal of the American Veterinary Medical Association, pp. 497-501.
Risler A, K. J. (2009, Mar -Apr). Puppy line, metaphyseal sclerosis, and caudolateral curvilinear and circumferential femoral head osteophytes in early detection of canine hip dysplasia. Vet Radiol and Ultrasound, pp. 157-66.
Runge JJ, K. S. (2010). Distraction index as a risk factor for osteoarthritis associated with hip dysplasia in four large dog breeds. Journal of Small Animal Practice, 264 -269.
Smith GK, B. D. (1990). New concepts of coxofemoral joint stability and the development of a clinical stress-radiographic method for quantitating hip joint laxity in the dog. Journal American Veterinary Medical Association, 59-70.
Smith GK, G. T. (1993, Jul 7). Coxofemoral joint laxity from distraction radiography and its contemporaneous and prospective correlation with laxity, subjective score, and evidence of degenerative joint disease from conventional hip-extended. J Vet Res, pp. 1021-42.
Smith GK, H. C. (1998, May 15). Reliability of the hip distraction index in two-month-old German Shepherd dogs. . J Am Vet Med Assoc,, pp. 1560-1563.
Smith GK, K. G.-L. (2012). Pathogenesis, Diagnosis, and Control of Canine Hip Dysplasia. In S. A. Karen M. Tobias, Veterinary Surgery: Small Animal (pp. 824-848). St. Louis: Elsevier.
Smith GK, L. D.-L. (2012, January 23). Chronology of Hip Dysplasia Development in a Cohort of 48 Labrador Retrievers Followed for Life. Veterinary Surgery, pp. 20-33.
Smith GK, M. P. (2001, Dec 15). Evaluation of risk factors for degenerative joint disease associated with hip dysplasia in German Shepherd Dogs, Golden Retrievers, Labrador Retrievers, and Rottweilers. J Am Vet Med Assoc, pp. 1719 -1724.
Smith GK, P. E., & McKelvie PF, K. R. (2006, Sept 1). Lifelong diet restriction and radiographic evidence of osteoarthritis of the hip joint in dogs. J Amer Vet Med Assoc, pp. 690-693.
Szabo SD, B. D. (2007, September 15). Evaluation of a circumferential femoral head osteophyte as an early indicator of osteoarthritis characteristic of canine hip dysplasia in dogs. Journal of the American Veterinary Medical Association, pp. 889-892.
Verhoeven G, F. R. (2012, Januray 23). Worldwide Screening for Canine Hip Dysplasia: Where AreWe Now? Veterinary Surgery, pp. 10-19.
WH, R. (1973). The dysplastic hip joint: its radiographic and histologic development. J Am Vet Radiol So, 35.
Witsberger TH, V. J. (2008, June 15). Prevalence of and risk factors for hip dysplasia and cranial cruciate ligament deficiency in dogs. J Am Vet Med Assoc, pp. 1818-1824.